Thyroid surgery is a common operation, but one which needs to be taken seriously
because of the potential complications which may occur. Commonly, this
surgery is done because of suspected cancer. Patient risk factors,
appearance on ultrasound examination or needle biopsy results may cause your
surgeon to recommend surgical removal of the thyroid. If there is a vocal cord
paralysis or rapid growth of a solid mass also indicates a cancer.
Unfortunately, one of the forms of thyroid cancer, follicular carcinoma, can
appear benign on needle biopsy and may also be read as benign on frozen section
during surgery. See
Evaluation of Thyroid Nodule Page
From 1973 to 2002 the incidence of thyroid cancer
has increase 2.4 times to 8.7 cases per 100,000 per year. The increase was
entirely due to an increase in papillary carcinoma. The mortality from
thyroid cancer has stayed unchanged at 0.5 patients per 100,000 per year.
View Article (JAMA 2006)
If the thyroid becomes so large that it compresses the
trachea
or
esophagus
surgical removal is indicated. A thyroid cyst
that recurs after a single or repeated needle drainage is also an indication for
removal. Rarely, a thyroiditis will cause scaring in
the neck which also compresses the airway. The thyroid must also be
removed in this case. However, cases of thyroiditis have an increased
complication rate due to bleeding and scaring.
The patient is positioned with the neck extended and a cloth roll placed under the shoulders.
A curvilinear stitch is outlined on the neck. The center portion is marked to better align the skin during closure.
The incision is carried through the superficial fascia and down to the anterior cervical veins which overlie the strap muscles.
Using scissor dissection, a superior skin flap is elevated in the plane above the anterior cervical veins.
A inferior flap is elevated in a similar fashion. Both the inferior and superior flaps must be elevated and elevated symmetrically. This is not only important for surgical exposure but also for the postoperative appearance of the neck by allowing the skin to drape over the neck without distortion.
The fascia between the strap muscles is divided in the midline.
The strap muscles are elevated, exposing the thyroid gland. There are no vessels in this plane.
Superficial inferior vessels are identified and ligated. As are the vessels which entered laterally and superiorly.
Dissection is usually carried out inferiorly to superiorly. This allows for identification and preservation of the recurrent laryngeal nerve (RLN).
Superiorly, a Kitner (peanut) dissector is used to push the fascia and soft tissue off the thyroid. This helps to protect and deflect the external branch of superior laryngeal nerve. In a similar fashion the superior thyroid artery and vein are exposed and ligated.
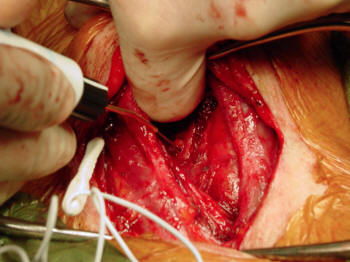
Shown here is the recurrent laryngeal nerve (RLN). It looks like a vein and before deep structures are cut, the RLN should be identified.
In this picture, the nerve is entering into a metastatic thyroid cancer nodule.
The gland is freed superiorly and the RLN is identified and traced down to where it enters the metastatic tumor mass.
A superior dissection is sometimes done first. This allows for increased exposure but can stretch the RLN between Berry's Ligament and where it enters the thyroid. This can result in a temporary or permanent laryngeal paralysis.
Both thyroid lobes were removed. The Recurrent Laryngeal Nerve can be seen on the left side.
The wound is irrigated and the patient was valsalved to check for bleeding. The strap muscles are closed. If these are not closed, the skin flaps will heal to the trachea and cause disturbing movement of the neck skin when the patient swallows.
The Superficial Cervical Fascia is closed.
The skin is closed with a 5-0 Nylon stitch. Some surgeons also use a subcuticular stitch.
Thyroid Surgery (Thyroidectomy) Care After Surgery:
Depending upon the working environment, patients can
expect to be off of work for one to three weeks. Stitches are removed in
five to seven days. If removed at five days, steri-strips are usually
applied to the incision. After 24 hours the incision can be gently
washed. Antibiotic ointment should be applied to the wound twice a day.
The wound must be kept clean.
Depending upon the diagnosis, thyroid medication
may be given. If only a single thyroid lobe is removed for benign
disease, and the opposite lobe is normal, then thyroid replacement is often not
started. If thyroiditis is present, then thyroid replacement should be
started.
If a total thyroidectomy is performed, thyroid replacement is mandatory.
If the thyroid was removed because of cancer, then thyroid suppressive dosages
should be considered. In cases of thyroid nodules, goiter and thyroiditis,
mild thyroid suppression is controversial because of the possible risk of
osteoporosis. If the patient is placed on thyroid suppression, a bone scan
for osteoporosis and supplemental calcium and vitamin D should be prescribed.
If I-131 therapy is planned after a total thyroidectomy, Cytomel (liothyronine
sodium), should be considered to shorten the time of hypothyroidism before the
treatment. Cytomel contains synthetic T3, a thyroid hormone with a
short half life. Thus, the patient is taken off of it for a shorter time
before I-131 therapy, than if the patient was prescribed a T4 replacement.
In all patients who receive thyroid replacement or suppression, TSH and Free-T4
should be routinely monitored. If hypoparathyroidism is suspected, calcium
levels will also need to be measured.
Thyroid Surgery (Thyroidectomy) Complications:
1) Paralysis of the
Recurrent Laryngeal Nerve(RLN) is
the most common complication after thyroid surgery. It can occur in
approximately 2% of patients. If one lobe of the thyroid is removed only
one RLN will be placed at risk. Injury can result in a weak, breathy
voice. However, in some patients compensation will occur and a strong
raspy voice results. In cases of a weak voice, augmentation of the vocal
cords may improve the voice.
If a total thyroidectomy is performed, both RLNs are
at risk. If both RLNs are injured, the patient will have a poor airway and may
require a
tracheotomy.
There is no satisfactory treatment for this
complication and the patient must decide between a strong voice and a good
airway, both are not possible.
The
picture to the right shows the appearance of the operative field after the
thyroid gland is removed. Note the left
recurrent laryngeal nerve. This
nerve runs next to the undersurface of the thyroid and between the
trachea
and
esophagus.
The
recurrent laryngeal nerve
controls the movement of
the left
true vocal cord. This nerve can be damaged during surgery, which will
result in a weak, breathy voice.
Mouse Over Picture to identify nerve.
Click on picture to enlarge.
2)
Hypoparathyroidism: There are four small glands next to the
thyroid which control calcium metabolism. These location of these glands
are variable and they can mimic lymph nodes and globs of fat. Two of
these glands are located on each side. If a total thyroidectomy is
performed (both the right and left thyroid lobes are removed) these glands may
be inadvertently removed. If all four are removed the patient's calcium
will drop over a matter of hours and cramps, tetany and cardiac arrest will
develop. Treatment is to give intravenous calcium. After
stabilization, the patient is discharged home on oral Vitamin D and calcium.
It must be stressed that these glands are hard to identify and one or two are
often removed during surgery. Repeated frozen section may be
required to identify the glands. If they can be identified after
removal, they can be implanted into the local muscles where they will grow and
calcium metabolism will return to normal after their function returns.
3) Bleeding: Because of the vascularity, bleeding can occur after
the operation which can cause airway obstruction. If this occurs, the
surgical wound must be opened immediately to relieve the pressure on the
trachea.
Google Ad space finances and sponsors
ENT USAtm Websites. ENT USAtm,
Cumberland Otolaryngology or Dr Kevin Kavanagh, MD do not endorse,
recommend, referrer to or are responsible for the Advertisements or
for the content or claims made in the Advertisements.



 The patient is positioned with the neck extended and a cloth roll placed under the shoulders.
The patient is positioned with the neck extended and a cloth roll placed under the shoulders. A curvilinear stitch is outlined on the neck. The center portion is marked to better align the skin during closure.
A curvilinear stitch is outlined on the neck. The center portion is marked to better align the skin during closure.  The incision is carried through the superficial fascia and down to the anterior cervical veins which overlie the strap muscles.
The incision is carried through the superficial fascia and down to the anterior cervical veins which overlie the strap muscles.  Using scissor dissection, a superior skin flap is elevated in the plane above the anterior cervical veins.
Using scissor dissection, a superior skin flap is elevated in the plane above the anterior cervical veins.  A inferior flap is elevated in a similar fashion. Both the inferior and superior flaps must be elevated and elevated symmetrically. This is not only important for surgical exposure but also for the postoperative appearance of the neck by allowing the skin to drape over the neck without distortion.
A inferior flap is elevated in a similar fashion. Both the inferior and superior flaps must be elevated and elevated symmetrically. This is not only important for surgical exposure but also for the postoperative appearance of the neck by allowing the skin to drape over the neck without distortion.  The fascia between the strap muscles is divided in the midline.
The fascia between the strap muscles is divided in the midline. The strap muscles are elevated, exposing the thyroid gland. There are no vessels in this plane.
The strap muscles are elevated, exposing the thyroid gland. There are no vessels in this plane. Superficial inferior vessels are identified and ligated. As are the vessels which entered laterally and superiorly.
Dissection is usually carried out inferiorly to superiorly. This allows for identification and preservation of the recurrent laryngeal nerve (RLN).
Superficial inferior vessels are identified and ligated. As are the vessels which entered laterally and superiorly.
Dissection is usually carried out inferiorly to superiorly. This allows for identification and preservation of the recurrent laryngeal nerve (RLN). Superiorly, a Kitner (peanut) dissector is used to push the fascia and soft tissue off the thyroid. This helps to protect and deflect the external branch of superior laryngeal nerve. In a similar fashion the superior thyroid artery and vein are exposed and ligated.
Superiorly, a Kitner (peanut) dissector is used to push the fascia and soft tissue off the thyroid. This helps to protect and deflect the external branch of superior laryngeal nerve. In a similar fashion the superior thyroid artery and vein are exposed and ligated. Shown here is the recurrent laryngeal nerve (RLN). It looks like a vein and before deep structures are cut, the RLN should be identified.
In this picture, the nerve is entering into a metastatic thyroid cancer nodule.
Shown here is the recurrent laryngeal nerve (RLN). It looks like a vein and before deep structures are cut, the RLN should be identified.
In this picture, the nerve is entering into a metastatic thyroid cancer nodule. The gland is freed superiorly and the RLN is identified and traced down to where it enters the metastatic tumor mass.
A superior dissection is sometimes done first. This allows for increased exposure but can stretch the RLN between Berry's Ligament and where it enters the thyroid. This can result in a temporary or permanent laryngeal paralysis.
The gland is freed superiorly and the RLN is identified and traced down to where it enters the metastatic tumor mass.
A superior dissection is sometimes done first. This allows for increased exposure but can stretch the RLN between Berry's Ligament and where it enters the thyroid. This can result in a temporary or permanent laryngeal paralysis. Both thyroid lobes were removed. The Recurrent Laryngeal Nerve can be seen on the left side.
Both thyroid lobes were removed. The Recurrent Laryngeal Nerve can be seen on the left side. The wound is irrigated and the patient was valsalved to check for bleeding. The strap muscles are closed. If these are not closed, the skin flaps will heal to the trachea and cause disturbing movement of the neck skin when the patient swallows.
The wound is irrigated and the patient was valsalved to check for bleeding. The strap muscles are closed. If these are not closed, the skin flaps will heal to the trachea and cause disturbing movement of the neck skin when the patient swallows. The Superficial Cervical Fascia is closed.
The Superficial Cervical Fascia is closed.  The skin is closed with a 5-0 Nylon stitch. Some surgeons also use a subcuticular stitch.
The skin is closed with a 5-0 Nylon stitch. Some surgeons also use a subcuticular stitch.















